What Upper Cross Syndrome Actually Is
Upper cross syndrome is a term coined by Czech neurologist Vladimir Janda to describe a predictable pattern of muscle imbalance in the neck, shoulders, and upper back. It is not a disease or a structural pathology. It is a postural pattern, a configuration the body falls into when certain muscles become chronically shortened and others become chronically lengthened and inhibited.
Understanding the pattern is the key to fixing it, because treating individual symptoms (neck pain, shoulder impingement, headaches) without addressing the underlying pattern is why so many people cycle through treatment without lasting improvement.
The Two Crosses
Janda described the pattern as an X shape when viewed from the side. One diagonal of the X runs from the front of the chest and anterior neck (tight) to the upper trapezius and levator scapulae (tight). The other diagonal runs from the deep cervical flexors (weak) to the lower trapezius and serratus anterior (weak).
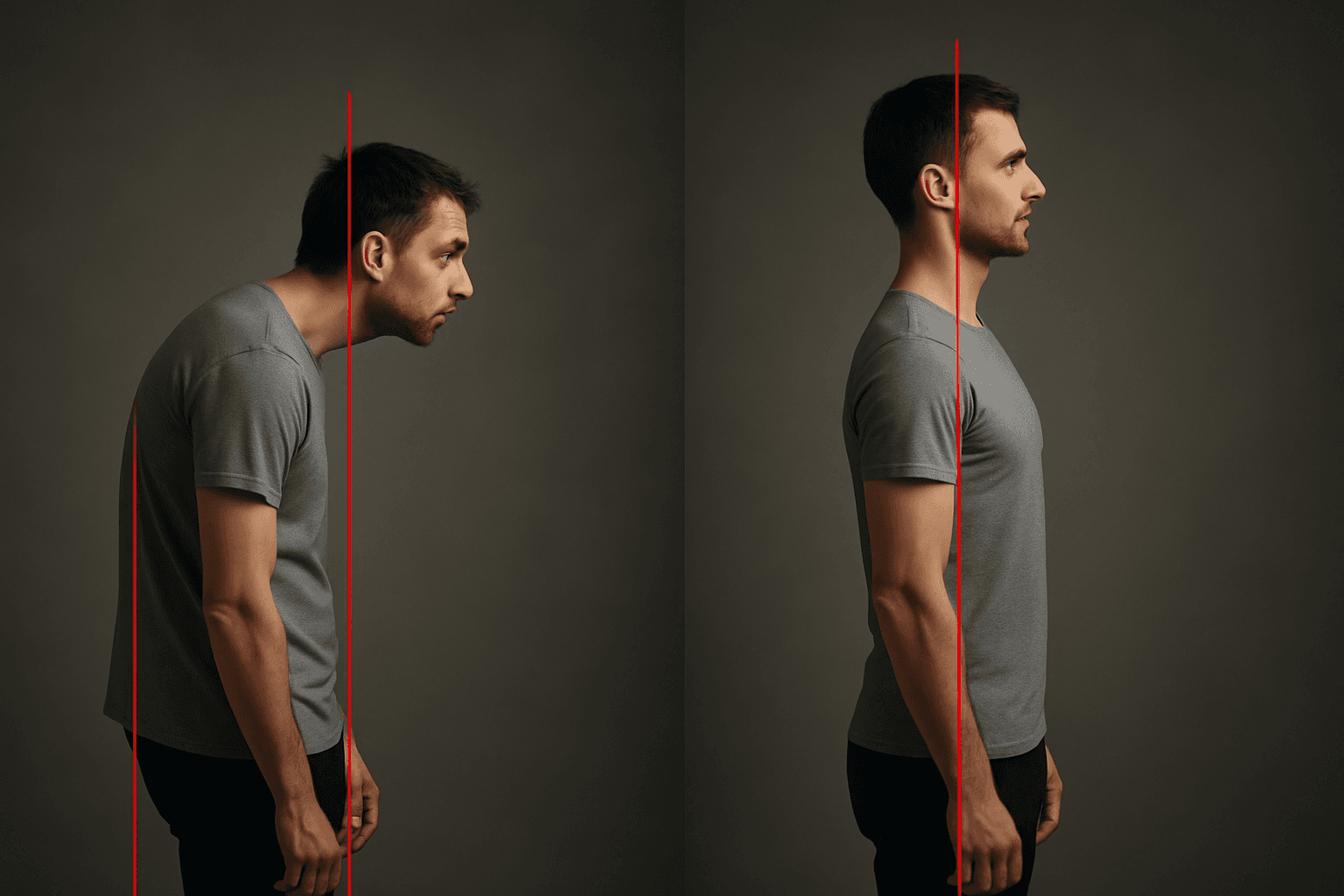
The tight muscles pull the head forward and up, round the shoulders forward, and elevate the shoulder blades. The weak muscles are the ones responsible for retracting and depressing the scapulae, and for maintaining a neutral head position against gravity.
The result is what most people recognize immediately: the combination of forward head posture, rounded shoulders, elevated and winged shoulder blades, and increased thoracic kyphosis.
How It Develops
Upper cross syndrome does not require an injury to develop. It develops through repeated positioning.
Sitting at a computer with the arms forward rounds the thoracic spine and loads the upper trapezius and levator scapulae. Looking at a screen positioned at or below eye level extends the cervical spine while the head moves forward, shortening the suboccipital muscles and the anterior cervical muscles simultaneously. Over hours per day and years, the nervous system registers these shortened positions as resting length and the lengthened muscles as chronically underutilized.
The progression is predictable. First, tightness develops in the pec minor, upper trapezius, and levator scapulae. Then the deep cervical flexors and lower trapezius become inhibited because they are chronically in an overstretched position. Then structural changes follow: the thoracic spine loses extension range, the cervical spine develops hyperlordosis to compensate, and the scapulae become fixed in an elevated, anteriorly tilted position.
Athletes are not exempt. Cyclists, swimmers, rock climbers, and overhead athletes develop upper cross syndrome from sport-specific positioning, often more severely than sedentary people because of the volume of time spent in provocative positions.
Why Standard Treatment Fails
Most people with upper cross syndrome receive treatment focused on the pain sites: neck massage, cervical manipulation, rotator cuff strengthening, or shoulder stretching. These treatments provide temporary relief because they address the tissue under tension, not the pattern creating the tension.
Tight upper trapezius muscles are tight because they are compensating for inhibited lower trapezius and serratus anterior. Stretching the upper trap provides relief until the next time the person sits at their desk for three hours. The compensation returns because the structural driver, the inhibited antagonists and the shortened anterior chain, was not addressed.
Effective correction requires releasing the tight structures and activating the inhibited ones in the right sequence. Release without activation leaves the body with no alternative pattern. Activation without release is fighting against shortened tissue.
Free - 60 seconds
Not sure which program you need?
Take the free posture quiz and get a personalized recommendation based on your pain and goals.
The Correction Sequence
Step 1: Release the Anterior Chain
The pec minor, anterior deltoid, and anterior neck muscles need to be lengthened before the posterior and stabilizing muscles can function properly. A doorway chest stretch at the level of the mid-chest, held for 60 to 90 seconds, targets the pec minor effectively. Corner stretches, with both arms at 90 degrees pressing into a corner, load both sides simultaneously.
Thoracic extension over a foam roller addresses the hyperkyphosis that locks the thoracic spine. This is the most critical release because scapular mechanics are directly dependent on thoracic mobility. No amount of shoulder work creates lasting change if the thoracic spine cannot extend.
Step 2: Activate the Deep Cervical Flexors
Cervical retraction, often called a chin tuck, re-engages the deep cervical flexors that are inhibited in upper cross syndrome. The key is precision: the movement is a horizontal glide of the head backward, not a downward tuck of the chin. This distinction matters because the downward movement does not target the deep flexors effectively.
Ten repetitions performed against a wall, with the back of the head sliding along the surface, provides proprioceptive feedback that helps the correct muscles activate. This exercise done consistently resets the resting position of the cervical spine over several weeks.
Step 3: Retrain Scapular Control
Prone YTW exercises target the lower trapezius and serratus anterior in a position where the upper trapezius cannot compensate. Lying face down removes the gravitational load that drives upper trap overactivation. The Y, T, and W positions progressively load different portions of the lower trapezius and rhomboids.
Wall angels, performed with the back, arms, and head in contact with a wall, train scapular retraction and depression while providing feedback about postural alignment. The wall prevents forward shoulder drift, which is the most common compensation.
Step 4: Integrate the Pattern
The goal of upper cross syndrome correction is not just to release tight muscles and strengthen weak ones. It is to change the movement pattern the nervous system defaults to. This requires repetition in functional positions.
Most people notice significant improvement in neck and shoulder tension within two to three weeks of consistent work. Structural change, meaning measurable improvement in resting head position and scapular mechanics, typically takes six to eight weeks.
The Forward Head Posture Fix program and Rounded Shoulders Fix program address upper cross syndrome systematically, working through the release and activation sequence in the order that produces lasting structural change rather than temporary symptomatic relief.

Mike Boshnack
Corrective Exercise Specialist · Posture Guy Mike
Mike Boshnack grew up skateboarding and surfing, trained MMA, and rode road bikes competitively. A shoulder injury put him on a path to discover corrective exercise. He has since helped thousands of people fix the structural patterns causing their pain, without surgery or passive treatments.
Keep Reading
Conditions & Pain
Why You Lean to One Side When You Sit or Stand (And How to Fix the Shift)
4 min read
Conditions & Pain
Should Your Toes Be Straight? The Truth About Toe Splay and Foot Health
8 min read
Conditions & Pain
Upper Back Pain Between Shoulder Blades: Why the Pain Is Not Where the Problem Is
7 min read
Related Conditions
Free tool
See where your posture stands right now.
Upload a photo and get an instant AI-powered posture analysis with personalized recommendations. Free, no account required.
Try the Free Posture CheckTake the next step
Fix the structural root cause, not just the symptom.
Mike's programs apply this corrective method to your specific condition. No gym, no equipment. Just a floor and 15 minutes. Buy once, own forever.
Discussion
Discussion is a Pro member feature. Visit the community for more.